Alright, sit down, shut up, and let me drop some divine dental wisdom on your soul. We’re talkin’ dental resorption—the silent, sneaky saboteur that don’t knock before comin’ in and wreckin’ your whole damn house. You ever see a tooth just… disappear? Like it’s bein’ eaten alive from the inside or the outside and no one invited you to the barbecue? That’s resorption, baby. And it doesn’t play fair.
The Aetiology – Or, Who Invited the Devil to Dinner?
Resorption don’t happen without a reason. There’s always a trigger man. Could be trauma—yeah, like that upper incisor you smashed on your bike in ’98. Could be infection—pulp goes necrotic, body sends in the cleanup crew, and boom, you got internal resorption. Or maybe it’s ortho—teeth movin’ too fast, roots don’t like that. You stress the system, the system fights back. And sometimes? It just happens. Idiopathic. That’s Latin for “God only knows.”
The Types – Know Thy Enemy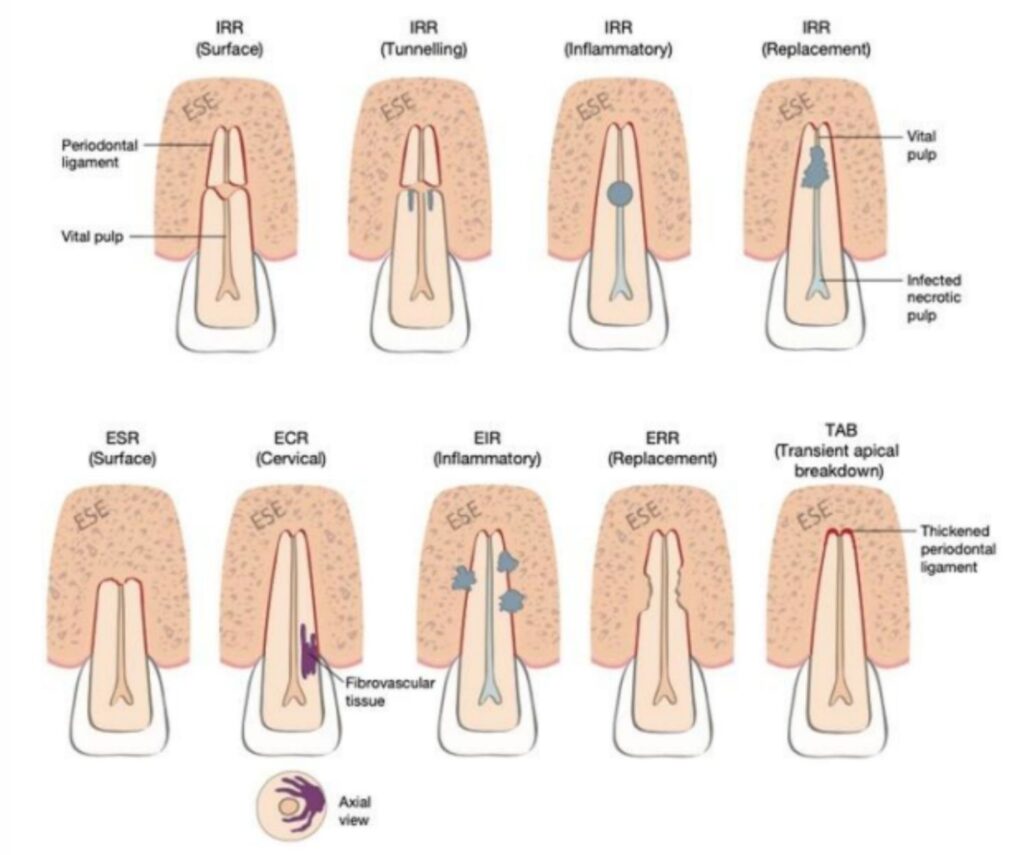
You got internal resorption—starts from the pulp, eats out the inside of the root like a termite in your floorboards. Pink spot on the crown? That ain’t cosmetics, that’s a warning light, brother

Internal resorption
Then you got external resorption—that’s the real horror movie stuff. Comes from the outside, like a SWAT team takin’ the wall down. Can be:
• Surface (small, self-limiting, mostly harmless—like a scratch on your car)
• Inflammatory (infection’s involved, and now we got a problem)
• Replacement (a.k.a. ankylosis—where your tooth literally fuses with bone, turns into a freakin’ fossil)
• Cervical resorption (hides right by the gumline, throws on a disguise and pretends to be decay—sneaky little punk)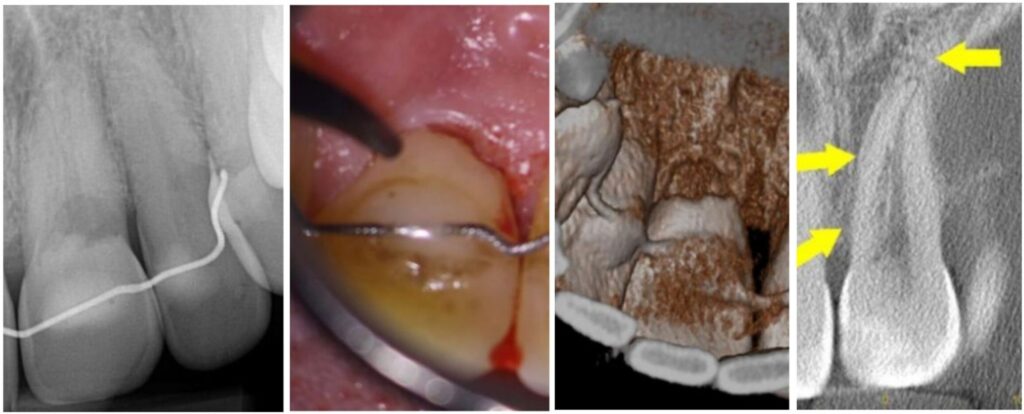
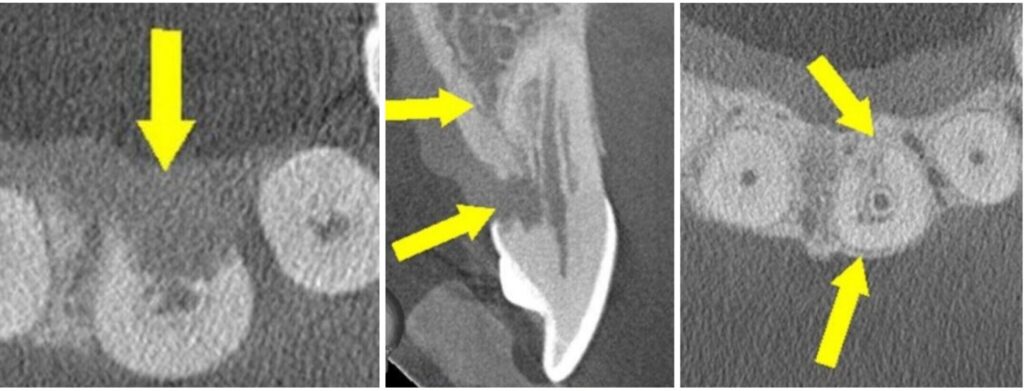 Cervical resortion: Note the apical extensions and circumpulpal spread
Cervical resortion: Note the apical extensions and circumpulpal spread
The Pathology – The Circle of Tooth Death
Here’s how it goes down: protective layers get damaged—cementum on the outside, predentin on the inside. That’s like leavin’ your door unlocked in a bad neighborhood. Then the clastic cells move in—odontoclasts, osteoclasts—and they ain’t here to make friends. They start resorbin’ mineralized tissue like they’re starvin’. Before you know it, your tooth structure’s dissolving like sugar in hot coffee.
The Management – Time to Lay Down the Law
Step one? Diagnosis. CBCT’s your best friend. Periapical radiographs can help, but CBCT? That’s like seein’ the Matrix. Don’t treat what you can’t see.
• Internal resorption? You better get that root canal done yesterday. Clean out the pulp, fill it tight, and hope the perforation fairy stayed home. Use warm vertical compaction, maybe some bioceramic magic if there’s a perforation.
• External inflammatory? Eliminate the source—usually infected pulp or periodontium. You’re doing RCT, maybe surgical access, maybe even MTA repair
if it’s gone rogue.
• Cervical resorption? Now that’s a game of strategy. You might be doin’ a surgical flap, trichloroacetic acid, curettage, restoration, prayer


Surigical cervical resoprtion MP UR6. NB repair only, RCT not required
• Replacement resorption (ankylosis)? Ain’t no stoppin’ that train. You monitor, maintain aesthetics, and when the tooth’s gone full Jurassic Park—extract and replace.
Final Sermon
You wanna treat resorption right? You need vision (that’s CBCT), you need a clinician with the judgment of Solomon and the hands of a watchmaker.
Don’t be fooled by subtle radiolucencies. That ain’t shadow—it’s the devil knocking. Resorption waits for no one. And remember: it ain’t about whether the lesion is big or small—it’s about whether the tooth has a future. And if it does… you better restore it like you mean it. If you diagnose early, act fast, and fight smart—you might just save that tooth’s soul.


