Winston Wolf Says: The Root Canal Isn’t Failing. Your Irrigation Is.
“Just because you prepared and shaped the canal doesn’t mean you’ve cleaned it.” Let’s get something straight. The rotary file is not the hero of root canal treatment. I know that’s disappointing. Dental companies have spent the last twenty years convincing us that if we buy the latest heat-treated, blue, gold, pink, reciprocating, adaptive-memory, moon-calibrated file system, endodontic success will magically follow. It won’t. Because files shape canals. Bacteria live somewhere else.
The Dirty Little Secret
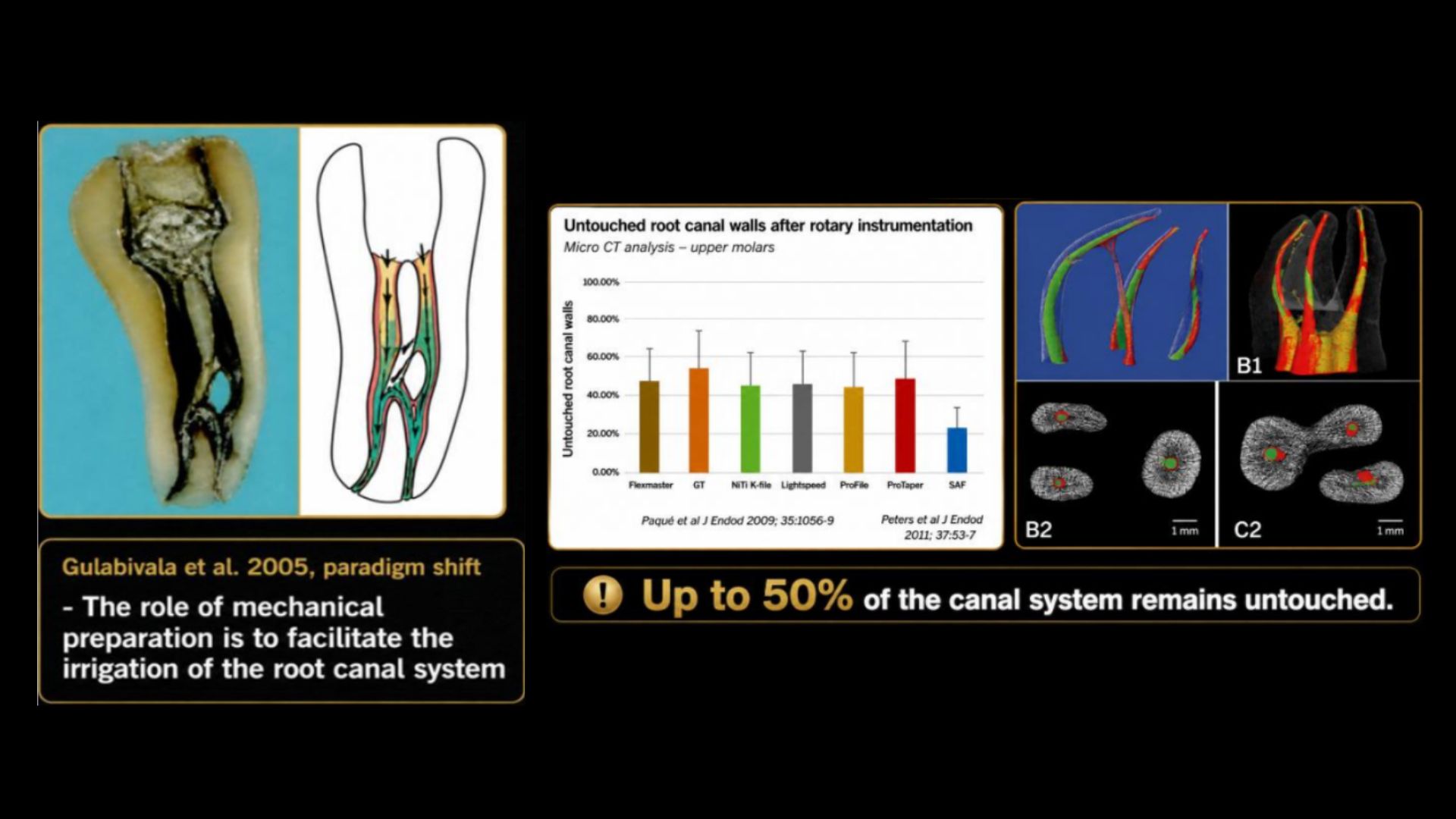
When you instrument a root canal, your file only contacts a fraction of the canal wall. Think about that for a moment. You may spend thirty minutes carefully shaping a canal to a beautiful taper, only to have touched less than half of the internal surface. The rest? Untouched. Uninstrumented. Still covered in biofilm. Still harbouring bacteria. Still plotting their revenge. If endodontics is fundamentally the management of infection, then irrigation is not an optional extra. It is the treatment. The files simply create a pathway that allows the irrigants to do their job. Or, as Winston Wolf might put it: “The files are the delivery system. The bleach is the assassin.”
Meet the MVP: Sodium Hypochlorite
Sodium hypochlorite (NaOCl) remains the gold standard irrigant. Nothing else comes close. It:
• Dissolves organic tissue
• Kills bacteria
• Disrupts biofilms
• Removes necrotic debris
• Penetrates areas instruments cannot reach
In other words, it does exactly what we need. And unlike many things in dentistry, it is cheap. The concentration debate continues to rage. 1%, 3%, 5%, 6%? The evidence increasingly suggests that volume, replenishment and activation may be more important than concentration alone. A fresh supply of 3% hypochlorite activated effectively will often outperform stronger stagnant bleach left sitting in the canal.
The key phrase is:
Fresh irrigant continuously delivered.
Once sodium hypochlorite reacts with tissue, it becomes exhausted. Like a boxer who has gone twelve rounds, it may still be standing, but it isn’t winning any more fights. Replace it. Frequently.
The Problem with the Syringe
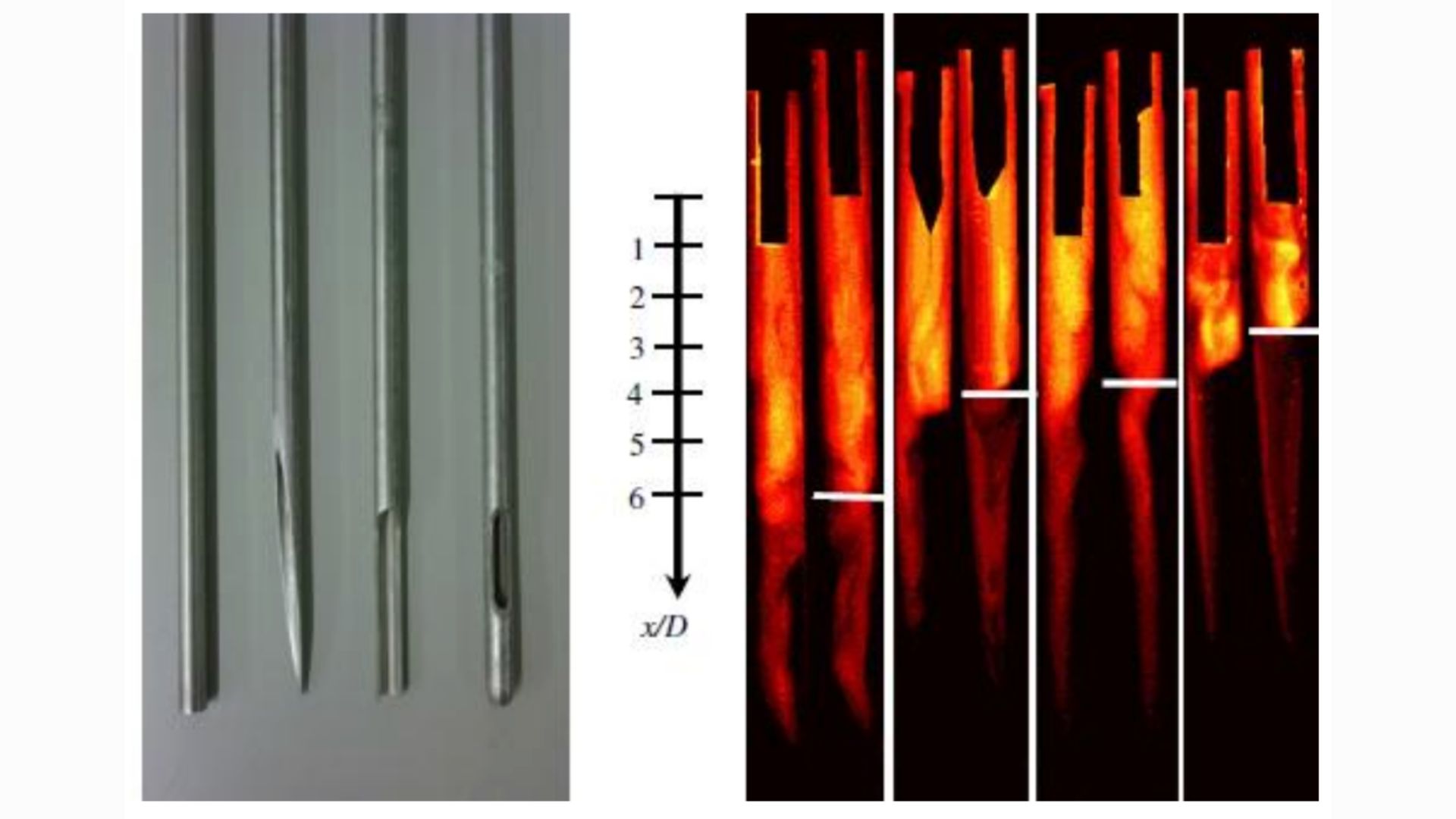
Most dentists irrigate like this: Insert needle. Squirt. Hope. Move on. Unfortunately, the irrigant does not share your optimism. Studies consistently show that conventional syringe irrigation penetrates only a limited distance beyond the needle tip. If the needle is sitting 8 mm short of working length, the apical third may barely see any fresh irrigant at all. Which is rather like washing only the top half of a dirty frying pan and declaring it clean. Needle position matters. Flow matters. Volume matters.
Time matters. Everything matters. Which brings us to activation.
Agitation Is Not Just For Teenagers
If irrigants are the cleaning solution, activation is the scrubbing brush. The goal is simple: Move fresh irrigant into places files cannot reach. This includes:
• Isthmuses
• Fins
• Lateral canals
• Oval extensions
• Recesses
• Apical complexities
In other words, all the places bacteria enjoy living.
And Then the Laser Walks Into the Room…
Every few years, endodontics gets excited about a new gadget. Some disappear quietly. Some become expensive coat hangers. And some genuinely change the game. Laser- assisted irrigation falls into the latter category. Before the pitchforks come out, let’s be clear: The laser is not replacing sodium hypochlorite. It is not replacing shaping. And it is certainly not replacing sound endodontic principles. What it can do is make your irrigants work much harder.
Why Lasers Matter
The challenge with irrigation has always been getting fresh irrigant into the complex
anatomy that files cannot touch. Remember:
• Isthmuses
• Fins
• Lateral canals
• Apical deltas
• Anastomoses
Nature did not design root canal systems to be cleaned. Lasers help by generating powerful fluid movement within the canal system. Instead of merely pushing irrigant up and down the main canal, laser energy creates rapid expansion and collapse of vapour bubbles. The result is a shockwave effect that drives irrigant throughout the canal system. Think less “gentle rinse.” Think more “pressure washer in a cave.”
Photoacoustic Streaming: The Clever Bit
Modern erbium lasers such as the LightWalker use a process known as photoacoustic
streaming. When the laser pulse interacts with the irrigant:
• Microscopic bubbles form
• These bubbles rapidly expand
• They then collapse
• Fluid movement accelerates dramatically
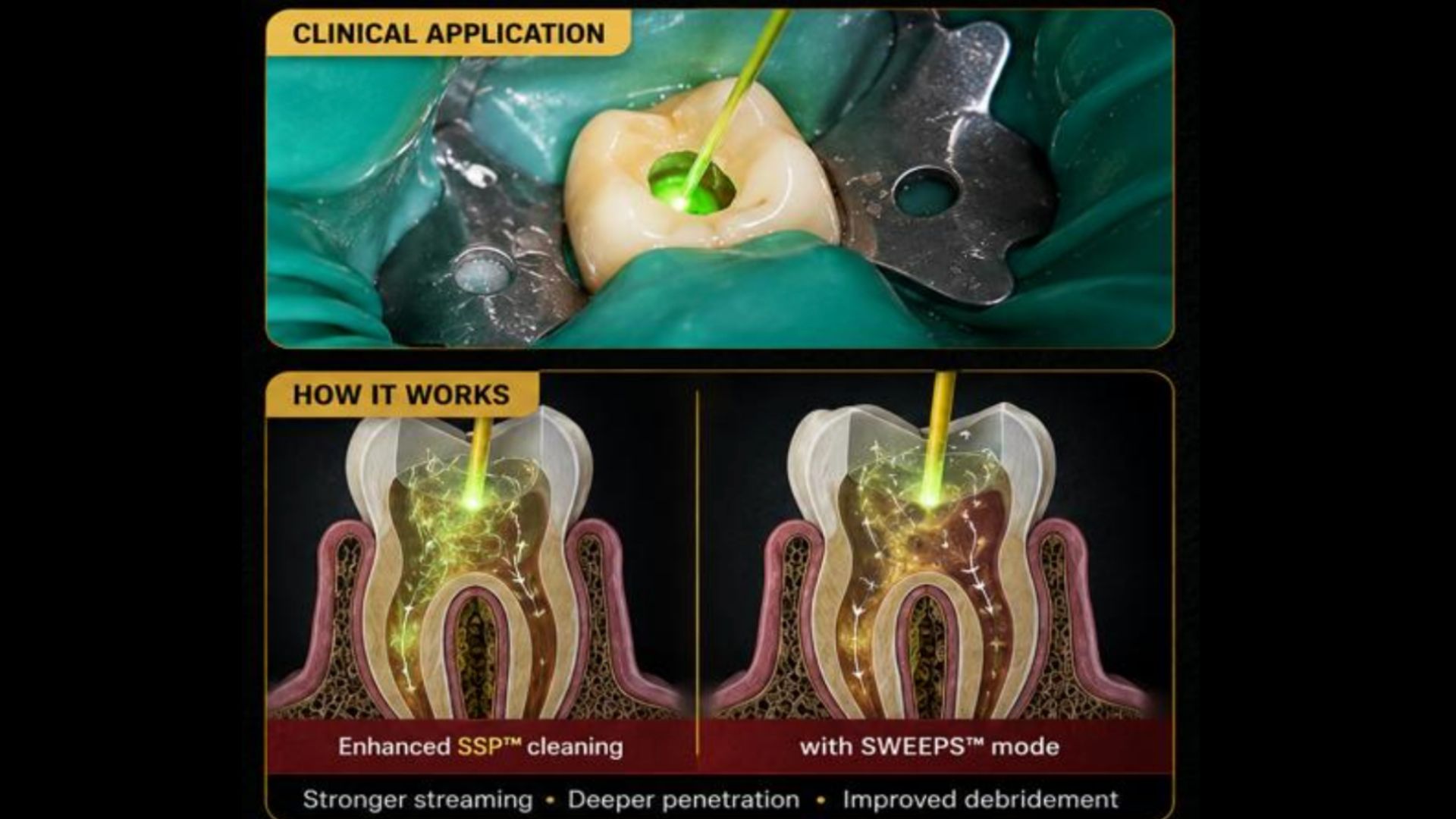
This creates powerful streaming effects throughout the canal system. Importantly, the laser tip does not need to be placed deep into the canal. In many protocols it remains in the pulp chamber. The energy is transferred to the irrigant, which then performs the cleaning. The irrigant remains the assassin. The laser simply gives it a much bigger weapon.
SWEEPS: The Next Generation
Perhaps the most exciting development is Shock Wave Enhanced Emission Photoacoustic Streaming (SWEEPS). The concept is beautifully simple. A second laser pulse is delivered at precisely the right moment to accelerate the collapse of the first bubble. This creates an even more powerful shockwave within the irrigant. The resulting fluid dynamics can reach areas that conventional activation methods may struggle to access. When viewed in slow-motion videos, it looks less like irrigation and more like controlled hydraulic violence. Exactly the sort of thing biofilms dislike.
Does It Actually Work?
The evidence is increasingly encouraging. Studies have demonstrated:
• Improved debris removal
• Better smear layer removal
• Enhanced penetration of irrigants
• Greater cleaning of isthmuses and complex anatomy
• Significant reductions in bacterial load
Particularly impressive results have been reported in molars with complex canal systems where traditional instrumentation leaves large areas untouched. Which, if we’re honest, is most molars. However, a note of caution. Laser activation does not overcome poor access. It does not compensate for missed canals. It does not rescue inadequate shaping. And it certainly does not fix a canal that was never found in the first place. The laser is an enhancer, not a magician.
The Winston Wolf Verdict
If conventional syringe irrigation is a garden hose… And ultrasonic activation is a pressure washer… Laser-assisted irrigation is probably a controlled explosion. It represents one of the most exciting advances in root canal disinfection over the past decade and is supported by an increasingly strong evidence base. Will every GDP need one? Probably not. Will every specialist practice eventually be using some form of advanced activation technology? Almost certainly. Because as our understanding of root canal anatomy improves, one thing becomes increasingly obvious: Success is not about touching more dentine. It is about cleaning anatomy that we cannot touch. And few technologies currently do that more effectively than laser-assisted irrigation. The files may create the shape. The irrigants may do the cleaning. But the laser? The laser turns up the volume.
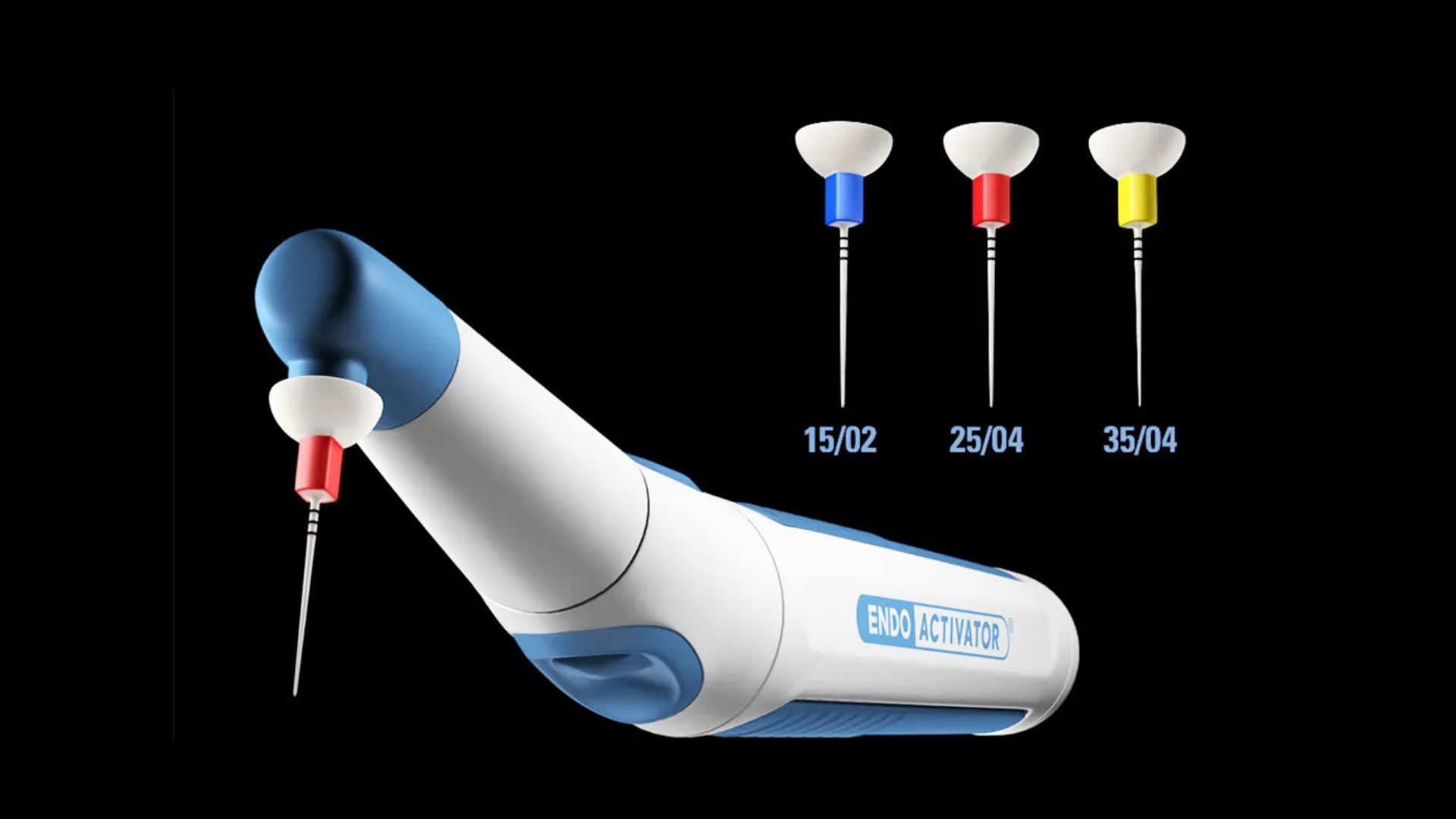
Sonic Activation
Systems such as EndoActivator use sonic energy to create fluid movement. Advantages:
• Easy to use
• Relatively inexpensive
• Safe
• Well supported by evidence
• It significantly improves irrigant penetration compared with syringe irrigation alone. For most GDPs, it represents one of the best upgrades available.
Ultrasonic Activation
Passive ultrasonic irrigation produces greater energy and more vigorous fluid movement.The oscillating ultrasonic tip generates acoustic streaming that can dramatically improve cleaning.
Advantages:
• Excellent evidence base
• Superior debris removal
• Improved biofilm disruption
Disadvantages:
• More technique sensitive
• Risk of touching canal walls
• Requires appropriate equipment
• When used correctly, it is extremely effective. When used incorrectly, it becomes an expensive way of scratching dentine.

The EDTA Conversation
Let’s discuss the smear layer. Every time you instrument a canal, you create a thin layer of organic and inorganic debris smeared across the canal wall. Imagine sanding a piece of wood and then rubbing the dust into every surface. That’s essentially what you’ve done. EDTA exists to remove the inorganic component of this smear layer.
Typically:
• 17% EDTA
• Approximately one minute
• Followed by a final rinse of sodium hypochlorite
This sequence opens dentinal tubules and improves cleanliness. It also allows your
sealer to interact more effectively with the canal wall. Think of EDTA as the cleaner that
removes the fingerprints before painting.
What About Chlorhexidine?
Let’s save everyone some time. Chlorhexidine is not sodium hypochlorite. It does not dissolve tissue. It does not replace sodium hypochlorite. It is not a miracle irrigant. Its antibacterial properties are useful, but in modern endodontics it has a very limited role. Many clinicians can perform an entire career of successful root canal treatment without
ever reaching for it.
How Much Irrigant Should You Use?
More than you currently are. Probably much more. Many successful endodontists routinely use:
• 20–30 ml per canal
• Sometimes considerably more in infected cases
This sounds excessive until you remember what you’re trying to achieve. You are attempting to disinfect a microscopic, anatomically complex bacterial ecosystem hidden inside a tooth. A few token squirts of bleach are unlikely to impress the microbes.
The Modern Irrigation Workflow
If Winston Wolf were performing your root canal, his workflow would probably look
something like this:
1. Establish glide path.
2. Begin shaping.
3. Irrigate frequently throughout instrumentation to flush out debris and prevent blockages.
4. Never allow canals to dry out.
5. Continuously replenish sodium hypochlorite.
6. Complete shaping.
7. Rinse with EDTA for 30 seconds per canal, activate where possible.
8. Final sodium hypochlorite rinse 3 x 30 seconds per canal.
9. Activate sodium hypochlorite.
10.Dry and obturate.
Simple. Predictable. Evidence-based. No magic.

The Bottom Line
The biggest mistake in endodontics is believing that instrumentation creates success. It doesn’t. The file creates access. The irrigant creates cleanliness. And cleanliness creates healing. The next time you finish shaping a beautiful canal and feel tempted to congratulate yourself, ask one question:
Have I actually cleaned it?
Because the bacteria don’t care what file system you used. They care whether the bleach reached them. And if it didn’t? They’ll be seeing you again in six months. Winston Wolf has spoken.


